
Image credit: Pexels via Pixabay
Recent research has shown that one in five deaths across the world is due to sepsis [1]. In the UK, it kills 52,000 people a year - more people than breast, bowel and prostate cancer combined. It is caused when a body’s immune response to an infection damages its own tissues and organs. Diagnosis is difficult, as the symptoms overlap with a range of other conditions. Treatment is with antibiotics and organ support, usually in an intensive care unit. The quicker the treatment starts, the better the outcomes. Globally, one-third of patients with sepsis don’t survive.
There are big questions that remain to be answered. Why do some people survive? How can doctors identify those who need to be rapidly moved into intensive care? Are there treatments that can target the immune system itself? Information from genomics might give clues, leading us towards precision medicine. Dr Emma Davenport, Group Leader at the Wellcome Sanger Institute is studying the genomics of the immune response in sepsis. She presented her work at the American Association for the Advancement of Science (AAAS) meeting in Seattle today.
Emma opened her talk with an introduction to DNA: “Any two people share more than 99 per cent of their DNA. It’s the remaining one per cent that makes us unique, contributes to susceptibility to disease, and how you respond to treatment,” she said.
“My group is really interested in how we can use genetic information to understand why there is such variation in both disease and response to treatment in cohorts of patients,” she said.
Emma described how cancer medicine has moved over the last few decades to incorporate genetic information. Angelia Jolie is one of many who has talked publicly about her experience of finding she has a genetic predisposition to breast and ovarian cancer, and her subsequent decision to have preventative surgery to reduce her risk.
Emma then described how small changes in DNA sequence can impact not only on someone’s disease risk but also on their response to a drug, such as warfarin. Warfarin is used as a blood thinner. Treatment usually requires someone to go into hospital, their progress to be monitored, and the dose adjusted accordingly. There have been genetic variations discovered in two genes that impact the way a person metabolises warfarin. Knowing which variant someone has can help determine the starting dose. “It’s not something you want to get wrong,” Emma said, “warfarin is also an ingredient of rat poison.”
“This kind of analysis works well when you have a small change in DNA sequence that leads to quite a big impact. But for many complex diseases, that’s not the case.”
“Our group is particularly interested in measuring gene expression as a method to try and understand this complex variation.” Emma described gene expression as being like a dimmer switch – each of the 20,000 genes in a cell can be switched off, or be on at different levels. Gene expression data can give researchers an idea of how a cell is functioning at any given point in time.

Sepsis
Emma’s research focuses on sepsis. “Anybody can develop sepsis,” she said. “It could start from an infected bite, a lung infection or a perforation in your intestines. A major challenge is that we don’t have a single diagnostic marker and sepsis can initially look like flu or a chest infection. It’s very hard to know who is just quite unwell, and who is rapidly going to decline and require intervention.”
“For the last 10 years I’ve been working on the genomic advances in sepsis study. We recruited patients from intensive care units (ICUs) around the UK; we now have over 1,000 patients. Blood samples were collected when they were admitted to the ICU.”
“We’ve generated gene expression data for this point in time, when the person is fighting the infection. From these data, we’re able to stratify our cohort into two groups, based on the genes that are active in their immune cells.”
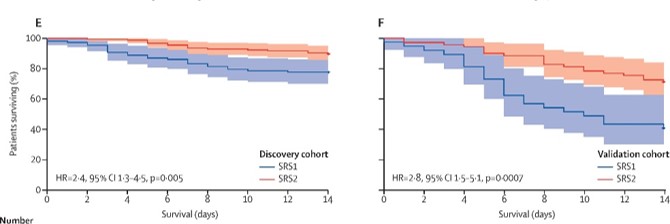
“We’ve started to explore the differences between these groups,” Emma said. “There is up and downregulation of genes, suggesting a different immune response in each group. The first group is immunosuppressed – their immune system is dampened down. And this group has a much higher mortality rate.”
“We’re now interested to know whether this has an impact on the way that people respond to treatments.”
Clinical trials
Clinical trials to test sepsis treatments have failed again and again over the years. Emma described part of the problem - trials are targeting such a diverse group of people. “The clinical definition of sepsis groups a lot of people together. We think actually we need to start subgrouping them down and seeing whether only certain people are going to respond to certain treatments.”
Emma has worked with collaborators undertaking clinical trials. The team analysed the gene expression signatures of patients who had taken part in a clinical trial to test the effectiveness of hydrocortisone, a steroid sometimes used in sepsis treatment. For people in group one – those with poorer outcomes - there was very little difference between those who were given the steroid and those who weren’t.
“However if we look at group two, they had a worse outcome,” Emma showed. She pointed out the number of patients in each group is small, meaning it is too soon to draw conclusions. “But this does highlight that individuals can have quite different responses to treatment, based on their gene expression levels at the point at which they are suffering from sepsis.”

“We are now interested in trying to expand this work to really understand how genetics is influencing this. Are people predestined to move into one of these groups or the other?” Emma asked. “Or are people cycling between these groups, in the balance of trying to fight the infection and then prevent damage from an over-active response?”
“We’re building up larger cohorts of patients where we have both genetic information and gene expression data over time, so we can find out,” Emma said. This project includes patients that are presenting to the emergency room with a suspected infection, as part of the BioAID study. They are going to be an even more varied group.
“We get an opportunity to have a look at gene expression very early, likely before any medical intervention. We are interested in whether the gene expression signatures might help to identify those individuals at most risk, and those that might benefit from intervention more quickly,” Emma said.
Emma ended by discussing precision medicine – if you can separate people into smaller and smaller groups, then you have the potential for treatments that are ever more tailored. Not personal – but precise, targeted and effective.

Links
- [1] https://www.sciencedirect.com/science/article/pii/S0140673619329897?via%3Dihub#bib1
- Emma’s BBC Expert Article
- Emma's profile and group website
- Bioresource in Adult Infectious Disease (BioAID)
- Genomic Advances in Sepsis (GAinS), GAinS Collaborator Anthony Gordon
Research papers:
- https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(16)00046-1/fulltext
- https://www.atsjournals.org/doi/full/10.1164/rccm.201608-1685OC



